Case Study: New York Life Group Benefit Solutions Transformed Medical Data into Insights with Medhub


Overcoming the Comorbidity Tax
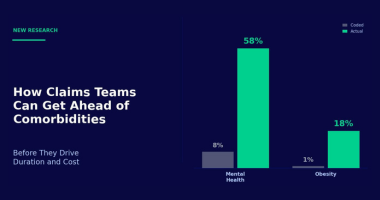
How Claims Teams Can Get Ahead of Comorbidities Before They Drive Duration and Cost

Every experienced adjuster knows that a knee injury or lumbar strain rarely tells the whole story. The real trajectory of a workers' comp claim is shaped by what lies beneath the surface: comorbidities like depression, obesity, chronic pain, and substance use that quietly compound recovery timelines and claim costs.
Your frontline teams already understand this. They see it in every complex file. The claimant whose straightforward rotator cuff repair stalls because untreated anxiety is keeping them from attending physical therapy. The back injury that won't close because underlying diabetes is slowing recovery. Adjusters have always known that comorbidities change outcomes. The problem is that the systems they rely on weren't built to help them act on that knowledge.
The Primary Diagnosis Trap
Most claims management systems were designed around structured fields and primary diagnosis codes. They index on the ICD code attached at first report and build workflows around that single data point. But injured workers don't arrive with a clean medical slate, and a primary diagnosis code captures only a fraction of what's actually driving the claim.
This creates what we call the primary diagnosis trap: the gap between what the system "sees" and what the adjuster knows is really happening. When your technology over indexes on structured diagnosis data, it misses the clinical complexity buried in physician notes, adjuster diaries, pharmacy records, and medical histories. That's the unstructured evidence where comorbidities actually live.
.webp)
Across our experience with over a million bodily injury and illness claims, we found 7 to 9 additional comorbidities hidden in unstructured data that never appear in the official codes. Mental health is the starkest example: while only 8% of claims carry a primary mental health diagnosis, 58% of claims contain a mental health comorbidity when unstructured records are analyzed. Obesity follows a similar pattern, appearing as a comorbidity in roughly 18% of injury claims but showing up as a primary diagnosis in less than 1%.
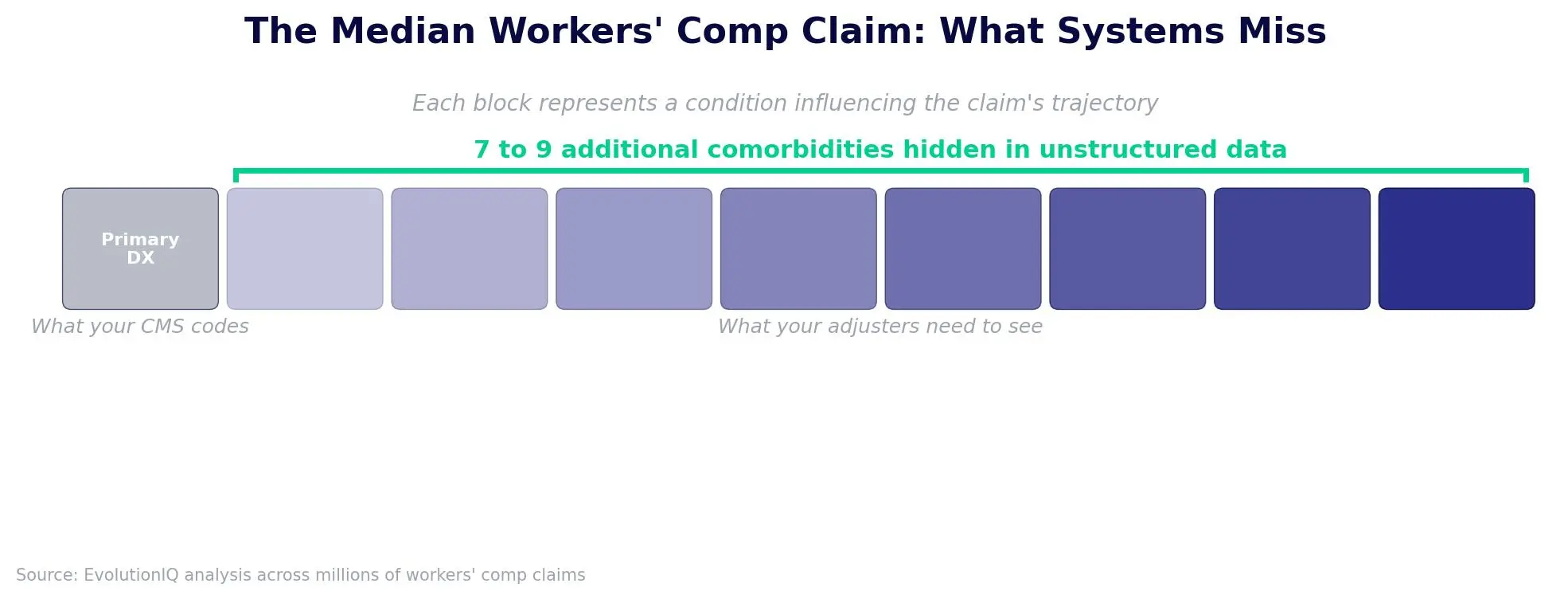
These aren't edge cases. They're the norm. And when your systems can't surface them systematically, your adjusters are left relying on experience and intuition to catch what the technology misses.
Why This Matters for Duration and Cost
Hidden comorbidities aren't just medical context. They're the primary drivers of claim stagnation and cost escalation.
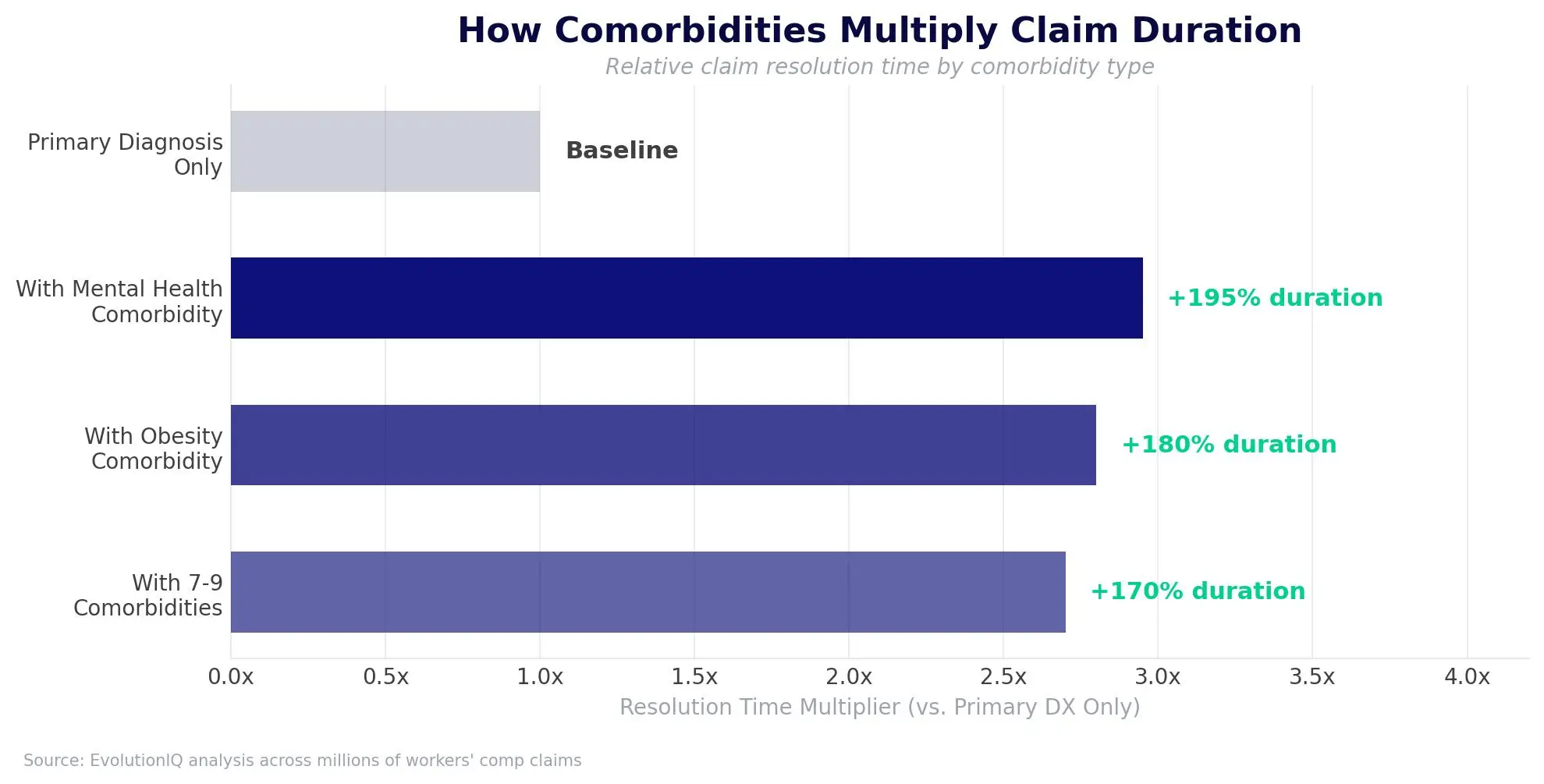
Claims with 7 to 9 comorbidities take approximately 2.7 times longer to resolve than those with only a primary diagnosis. Mental health conditions can stretch claim durations by 195%. Obesity can increase closure times by 180%.
For claims leaders managing loss ratios and reserve accuracy, these aren't abstract statistics. They represent the claims that quietly deteriorate in an adjuster's book. Not because the adjuster doesn't care, but because the system didn't flag the risk early enough to intervene. By the time the reserve gets bumped and the file gets escalated, the window for the most effective interventions has often closed.
Empowering Adjusters to Act on What They Already Know
The solution isn't asking adjusters to work harder or review more files. It's giving them systems that match their clinical awareness. Technology that ingests both structured and unstructured data continuously, surfaces comorbidity signals in real time, and translates those signals into specific next-best-actions.
This is the shift from reactive claims administration to proactive claims guidance. Instead of catching comorbidity-driven complications after a claim has stalled, adjusters can identify risk factors at first report and throughout the life of the claim. That means earlier specialist referrals, more targeted return-to-work plans, and interventions timed to when they'll actually change the trajectory, not after the trajectory has already been set.
When frontline teams are equipped with claims-specific medical intelligence (not just generic summarization, but insight that connects comorbidity patterns to claims outcomes) they can do what they've always wanted to do: act as recovery advocates from day one, with the data to back up their judgment.
The carriers that close the gap between what their adjusters know and what their systems can see are the ones that will control duration, protect margins, and deliver better outcomes for injured workers. The question isn't whether comorbidities matter. Your teams already know they do. The question is whether your technology is built to help them act on it.
Related posts


.png)

AI powered Claims Guidance.


